CAR-T therapy has delivered remarkable clinical outcomes, yet scaling manufacturing remains one of the industry's greatest challenges. Learn why CAR-T isn't simply selling engineered cells—it's selling an entire vein-to-vein supply chain


One question frequently comes up when discussing CAR-T therapy:
If CAR-T delivers such extraordinary clinical outcomes, why hasn't it achieved the same widespread adoption as monoclonal antibodies or GLP-1 therapies?
The answer isn't efficacy, it's manufacturing. More specifically, it's the inability to achieve economies of scale.
Unlike conventional biologics, CAR-T companies are not simply manufacturing bags of engineered T cells. They are delivering an end-to-end vein-to-vein supply chain.
That distinction explains why scaling CAR-T has proven far more difficult than scaling almost any other class of biologic therapies.
When CAR-T entered the market in 2017, it represented one of the most significant breakthroughs in modern oncology.
Both Kymriah from Novartis and Yescarta from Kite Pharma, a Gilead Sciences company, demonstrated overall response rates exceeding 80% in clinical trials.
For patients with relapsed or refractory hematologic malignancies who had exhausted conventional treatment options, CAR-T proved for the first time that the immune system could be genetically reprogrammed into a powerful anti-cancer therapy.
The science worked. The market, however, proved far more challenging.
Commercial adoption progressed much more slowly than many had expected—not because the therapy lacked efficacy, but because manufacturing proved extraordinarily difficult.
In its early commercial years, Kymriah's biggest competitor wasn't another CAR-T product, it was its own manufacturing process.
Because autologous CAR-T uses each patient's own T cells, every treatment represents a completely independent manufacturing batch. Early in commercialization, Novartis experienced relatively high manufacturing failure rates.
Some patient-derived T cells failed to expand sufficiently. Others couldn't meet GMP release specifications and therefore could not be released for clinical use.
For patients, this wasn't simply a manufacturing defect. It was a race against time. Many patients waited three to four weeks after leukapheresis before their engineered cells were ready for infusion.
Receiving news that manufacturing had failed didn't merely mean losing a product. It could mean losing the patient's final opportunity for treatment.
By comparison, Yescarta demonstrated greater manufacturing consistency during its early launch, helping it gain market share more rapidly.
Kymriah ultimately taught the entire industry an important lesson:
The challenge of CAR-T isn't only scientific innovation—it is manufacturing reliability.
Manufacturing stability was only the beginning; the real challenge was scalability.
For most biologics, increasing demand is relatively straightforward. Companies build larger facilities, install additional production lines, or expand bioreactor capacity.
Higher production volumes reduce unit costs through economies of scale.
However, CAR-T works differently. Because every therapy is individually manufactured for a single patient, CAR-T behaves less like a standardized pharmaceutical product and more like a highly specialized manufacturing service. Every patient requires an entirely new production cycle.
This complete journey—from collecting a patient's cells to returning the final engineered product—is known as the vein-to-vein process.
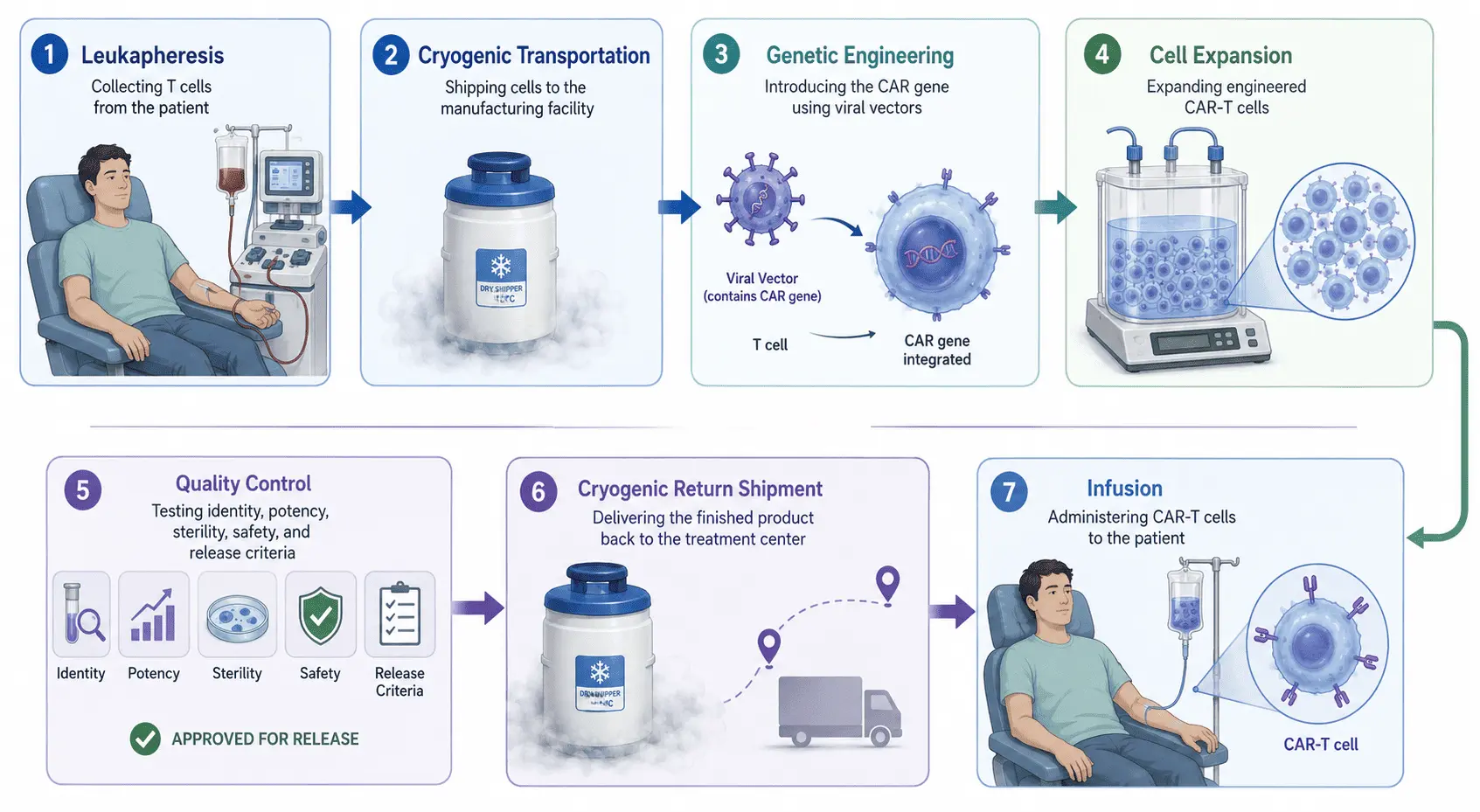

The process typically includes:
Although these steps appear straightforward on paper, each introduces additional time, cost, operational complexity, and manufacturing risk.
CAR-T companies are therefore selling far more than engineered cells. They are delivering an integrated, highly coordinated supply chain.
This fundamental principle distinguishes CAR-T from virtually every other pharmaceutical product.
Consider monoclonal antibodies.
A single 2,000-liter bioreactor batch may produce enough drug to treat thousands—or even tens of thousands—of patients. (It depends on yield rate, of course) Higher production volumes lower manufacturing costs. That's the essence of economies of scale.
Autologous CAR-T follows the exact opposite model. Every additional patient requires:
The company isn't simply producing more product; it's repeating the entire manufacturing process. This is why autologous CAR-T offers virtually no traditional economies of scale.
Within the cell therapy industry, one phrase summarizes the business model perfectly:
One Patient. One Batch.
These four words largely define the cost structure of autologous CAR-T. Every additional patient requires additional investment in:
Among these, GMP manufacturing and quality control represents one of the largest cost drivers. Every batch must independently verify:
None of these tests disappear simply because production volume increases.
Consequently, the cost of goods (COGS) for CAR-T remains significantly higher than that of conventional biologics.
Even with treatment prices reaching several hundred thousand dollars per patient, gross margins are often lower than many outsiders assume.
Once the industry recognized that "One Patient, One Batch" was the fundamental bottleneck, the next question naturally emerged:
If manufacturing—not science—is what truly limits the growth of CAR-T, can the business model itself be redesigned?
This question has become one of the defining themes in the evolution of cell therapy.
Whether it's allogeneic CAR-T or in vivo CAR-T, the goal is not merely to overcome technical challenges. These next-generation approaches aim to solve the fundamental limitation of autologous CAR-T: its inability to scale efficiently.
The future of CAR-T will therefore be shaped by more than better CAR designs.
The real competition will be about who can build a manufacturing and supply chain platform that is scalable, cost-efficient, and capable of supporting global commercialization.
In other words, the next breakthrough in CAR-T may not come from biology alone. It may come from a Better CARs. and Better business models. That's the future I'm most excited about.


